Discussion: Posterior Humeral Dislocation
The glenohumeral joint is relatively unstable and its dislocations can be classified
into anterior, posterior, superior, and inferior types. Anterior dislocation
is the most common, and the remaining dislocations are rare. Posterior dislocation
accounts for only about 2 to 4% of shoulder dislocations It often goes unrecognized
on initial evaluation, especially when only view of the shoulder is obtained.
Therefore, the physician should order a lateral scapular projection or an
axillary projection in addition to the anteroposterior view whenever dislocation
is suspected.
The mechanism of injury involves directly applied force to the arm while the
shoulder is flexed, adducted, and internally rotated. It takes great force
to cause such an injury, and therefore it is usually seen in patients who underwent
seizures or sustained an electrical burn. Convulsions may lead to bilateral
dislocations. Physical exam shows that the humeral head is displaced posteriorly
and internally rotated.
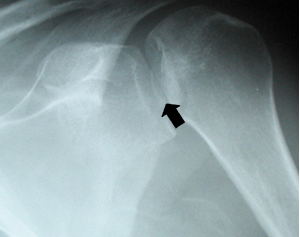
On the AP view, the following radiographic signs can be appreciated:
1. Distortion of the normal elliptical radiodense area created by overlapping of the humeral head and glenoid fossa.
2. A vacant glenoid cavity.
![]()
3. Loss of parallelism between the articular surfaces of the glenoid cavity and humeral head.
4. Internal rotation of the humerus.
5. Impaction fracture, also called the trough line, which is a second cortical
line parallel and lateral to the subchondral articular surface of the humeral
head.
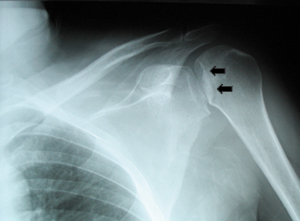
On the axillary view:
1. Posterior displacement of the humeral head.
2. Trough line.

Sources:
1. Gay, Spencer B. and Richard J. Woodcock, Jr. Radiology Recall, 2000.
2. Resnick, Donald. Diagnosis of Bone and Joint Disorders, 3rd Ed. Philadelphia:
W.B.Saunders Company, 1995.