 Paleopathological Evidence
Paleopathological Evidence
Although
abundant documentary evidence for smallpox in antiquity exists, physical
evidence is scant. The most striking
indication of the disease is found in mummies.
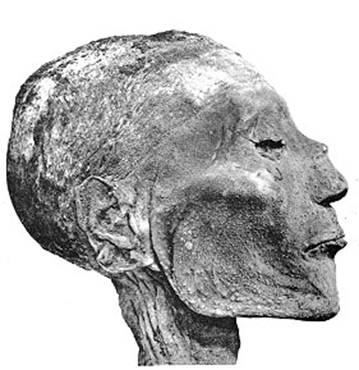
The mummy of Egyptian Pharaoh Ramses V, who was in his early thirties
when he died in 1157 B.C., exhibited a pustular rash on the face, neck,
shoulders and arms. Donald Hopkins, a
physician and epidemiologist who was permitted to partially examine this mummy
in 1979, describes a “rash of elevated ‘pustules,’ each about two to four
millimeters in diameter...pale yellow against a dark brown-reddish background”
(1983, 15). The image of the pharaoh’s face, covered in pustular-looking
lesions, can be found in much of the literature addressing the history of
smallpox.
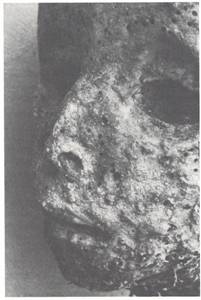 At least one attempt
to positively identify smallpox in mummies, however, was successful. Fornaciari and Marchetti (1986), utilizing an
immunological assay, were able to identify smallpox as the agent responsible for
the pustular lesions on a sixteenth century child’s mummy from
At least one attempt
to positively identify smallpox in mummies, however, was successful. Fornaciari and Marchetti (1986), utilizing an
immunological assay, were able to identify smallpox as the agent responsible for
the pustular lesions on a sixteenth century child’s mummy from
Skeletal evidence of smallpox in antiquity,
however, is not so apparent. Although,
as mentioned previously, joint lesions can occur in smallpox infections, it is
possible that in skeletal remains it would be difficult to differentiate such
pathology from other degenerative joint diseases. Cohen (1989, 108), in discussing skeletal
evidence in prehistoric remains for various infectious diseases, asserts that
identification of smallpox is controversial, but that it “may be identifiable
from patterns of inflammation on the ulna.”
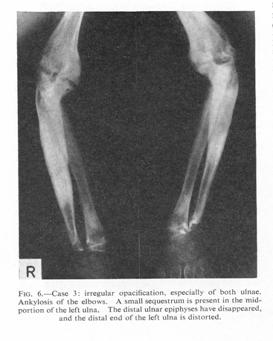 Evidence in modern
populations is more apparent, and a pattern is clear. Eekels et al. (1964) reported three cases of
osteomyelitis variolosa seen during a smallpox epidemic that occurred in the Republic
of the
Evidence in modern
populations is more apparent, and a pattern is clear. Eekels et al. (1964) reported three cases of
osteomyelitis variolosa seen during a smallpox epidemic that occurred in the Republic
of the
Ortner and Putschar (1981, 228) report
similar findings from work done in
 Return home
Return home